Our feet are constantly under stress. It’s no wonder that 80 percent of us will have some sort of problem with our feet at some time or another. Many things affect the condition of our feet: activity level, occupation, other health conditions, and perhaps most importantly, shoes. Many of the problems that arise in the foot are directly related to shoes, so it is very important to choose shoes that are good for your feet.
The foot is an incredibly complex mechanism. This introduction to the anatomy of the foot will not be exhaustive but rather highlight the structures that relate to conditions and surgical procedures of the foot.
Important Structures
The important structures of the foot can be divided into several categories. These include
- bones and joints
- ligaments and tendons
- muscles
- nerves
- blood vessels
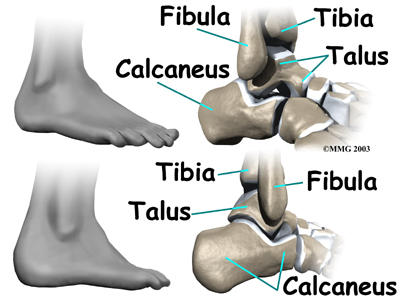
Bones and JointsThe skeleton of the foot begins with the talus, or ankle bone, that forms part of the ankle joint. The two bones of the lower leg, the large tibia and the smaller fibula, come together at the ankle joint to form a very stable structure known as a mortise and tenon joint.
The mortise and tenon structure is well known to carpenters and craftsmen who use this joint in the construction of everything from furniture to large buildings. The arrangement is very stable.
The two bones that make up the back part of the foot (sometimes referred to as the hindfoot) are the talus and thecalcaneus, or heelbone. The talus is connected to the calcaneus at the subtalar joint. The ankle joint allows the foot tobend up and down. The subtalar joint allows the foot to rock from side to side.
Just down the foot from the ankle is a set of five bones called tarsal bones that work together as a group. These bones are unique in the way they fit together. There are multiple joints between the tarsal bones. When the foot is twisted in one direction by the muscles of the foot and leg, these bones lock together and form a very rigid structure. When they are twisted in the opposite direction, they become unlocked and allow the foot to conform to whatever surface the foot is contacting.
The tarsal bones are connected to the five long bones of the foot called the metatarsals. The two groups of bones are fairly rigidly connected, without much movement at the joints.
Finally, there are the bones of the toes, the phalanges. The joints between the metatarsals and the first phalanx is called the metatarsophalangeal joint (MTP). These joints form the ball of the foot, and movement in these joints is very important for a normal walking pattern. Not much motion occurs at the joints between the bones of the toes. The big toe, or hallux, is the most important toe for walking, and the first MTP joint is a common area for problems in the foot.
Ligaments and TendonsLigaments are the soft tissues that attach bones to bones. Ligaments are very similar to tendons. The difference is that tendons attach muscles to bones. Both of these structures are made up of small fibers of a material called collagen. The collagen fibers are bundled together to form a rope-like structure. Ligaments and tendons come in many different sizes, and like rope, are made up of many smaller fibers. The thicker the ligament (or tendon) the stronger the ligament (or tendon) is.
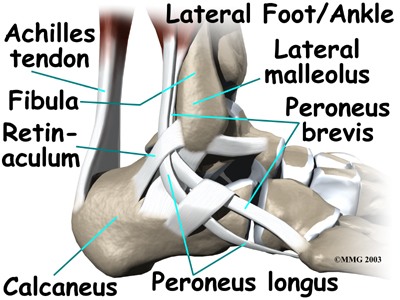
The large Achilles tendon is the most important tendon for walking, running, and jumping. It attaches the calf muscles to the heel bone to allow us to raise up on our toes. The posterior tibial tendon attaches one of the smaller muscles of the calf to the underside of the foot. This tendon helps support the arch and allows us to turn the foot inward. The toes have tendons attached that bend the toes down (on the bottom of the toes) and straighten the toes (on the top of the toes). The anterior tibial tendon allows us to raise the foot. Two tendons run behind the outer bump of the ankle (called the lateral malleolus) and help turn the foot outward.
Many small ligaments hold the bones of the foot together. Most of these ligaments form part of the joint capsulearound each of the joints of the foot. A joint capsule is a watertight sac that forms around all joints. It is made up of the ligaments around the joint and the soft tissues between the ligaments that fill in the gaps and form the sac.
MusclesMost of the motion of the foot is caused by the stronger muscles in the lower leg whose tendons connect in the foot. Contraction of the muscles in the leg is the main way that we move our feet to stand, walk, run, and jump.
There are numerous small muscles in the foot. While these muscles are not nearly as important as the small muscles in the hand, they do affect the way that the toes work. Damage to some of these muscles can cause problems.
Most of the muscles of the foot are arranged in layers on the sole of the foot (the plantar surface). There they connect to and move the toes as well as provide padding underneath the sole of the foot.
NervesThe main nerve to the foot, the tibial nerve, enters the sole of the foot by running behind the inside bump on the ankle, the medial malleolus. This nerve supplies sensation to the toes and sole of the foot and controls the muscles of the sole of the foot. Several other nerves run into the foot on the outside of the foot and down the top of the foot. These nerves primarily provide sensation to different areas on the top and outside edge of the foot.
Blood VesselsThe main blood supply to the foot, the posterior tibial artery, runs right beside the nerve of the same name. Other less important arteries enter the foot from other directions. One of these arteries is the dorsalis pedis that runs down the top of the foot. You can feel your pulse where this artery runs in the middle of the top of the foot.
he ankle joint acts like a hinge. But it’s much more than a simple hinge joint. The ankle is actually made up of several important structures. The unique design of the ankle makes it a very stable joint. This joint has to be stable in order to withstand 1.5 times your body weight when you walk and up to eight times your body weight when you run.
Normal ankle function is needed to walk with a smooth and nearly effortless gait. The muscles, tendons, and ligaments that support the ankle joint work together to propel the body. Conditions that disturb the normal way the ankle works can make it difficult to do your activities without pain or problems.
This guide will help you understand
- what parts make up the ankle
- how the ankle works
Important Structures
The important structures of the ankle can be divided into several categories. These include
- bones and joints
- ligaments and tendons
- muscles
- nerves
- blood vessels
The top of the foot is referred to as the dorsal surface. The sole of the foot is the plantar surface.
Bones and Joints
The ankle joint is formed by the connection of three bones. The ankle bone is called the talus. The top of the talus fits inside a socket that is formed by the lower end of the tibia (shinbone) and the fibula (the small bone of the lower leg). The bottom of the talus sits on the heelbone, called the calcaneus.
The talus works like a hinge inside the socket to allow your foot to move up (dorsiflexion) and down (plantarflexion). Woodworkers and craftsmen are familiar with the design of the ankle joint. They use a similar construction, called amortise and tenon, to create stable structures. They routinely use it to make strong and sturdy items, such as furniture and buildings.
Inside the joint, the bones are covered with a slick material called articular cartilage. Articular cartilage is the material that allows the bones to move smoothly against one another in the joints of the body.
The cartilage lining is about one-quarter of an inch thick in most joints that carry body weight, such as the ankle, hip, or knee. It is soft enough to allow for shock absorption but tough enough to last a lifetime, as long as it is not injured.
Ligaments and Tendons
Ligaments are the soft tissues that attach bones to bones. Ligaments are very similar to tendons. The difference is that tendons attach muscles to bones. Both of these structures are made up of small fibers of a material called collagen. The collagen fibers are bundled together to form a rope-like structure. Ligaments and tendons come in many different sizes and like rope, are made up of many smaller fibers. Thickness of the ligament or tendon determines its strength.
Ligaments on both sides of the ankle joint help hold the bones together. Three ligaments make up the lateral ligament complex on the side of the ankle farthest from the other ankle. (Lateral means further away from the center of the body.) These include the anterior talofibular ligament (ATFL), the calcaneofibular ligament(CFL), and the posterior talofibular ligament (PTFL). A thick ligament, called the deltoid ligament, supports the medial ankle (the side closest to your other ankle).
Ligaments also support the lower end of the leg where it forms a hinge for the ankle. This series of ligaments supports the ankle syndesmosis, the part of the ankle where the bottom end of the fibula meets the tibia. Three main ligaments support this area. The ligament crossing just above the front of the ankle and connecting the tibia to the fibula is called the anterior inferior tibiofibular ligament (AITFL). The posterior fibular ligaments attach across the back of the tibia and fibula. These ligaments include the posterior inferior tibiofibular ligament (PITFL) and the transverse ligament. The interosseous ligament lies between the tibia and fibula. (Interosseous means between bones.) The interosseus ligament is a long sheet of connective tissue that connects the entire length of the tibia and fibula, from the knee to the ankle.
The ligaments that surround the ankle joint help form part of the joint capsule. A joint capsule is a watertight sac that forms around all joints. It is made up of the ligaments around the joint and the soft tissues between the ligaments that fill in the gaps and form the sac.
The ankle joint is also supported by nearby tendons. The large Achilles tendon is the most important tendon for walking, running, and jumping. It attaches the calf muscles to the calcaneus (heelbone) and allows us to raise up on our toes. The posterior tibial tendon attaches one of the smaller muscles of the calf to the underside of the foot. This tendon helps support the arch and allows us to turn the foot inward. The anterior tibial tendon allows us to raise the foot. Two tendons run behind the outer bump of the ankle (the lateral malleolus). These two tendons, called the peroneals, help turn the foot down and out.
Muscles Most of the motion of the ankle is caused by the stronger muscles in the lower leg whose tendons pass by the ankle and connect in the foot. Contraction of the muscles in the leg is the main way that we move our ankle when we walk, run, and jump.
The key ankle muscles have been discussed earlier in the section on ligaments and tendons. These muscles and their actions are also listed here.
- The peroneals (peroneus longus and peroneus brevis) on the outside edge of the ankle and foot bend the ankle down and out.
- The calf muscles (gastrocnemius and soleus) connect to the calcaneus by the Achilles tendon. When the calf muscles tighten, they bend the ankle down.
- The posterior tibialis muscle supports the arch and helps turn the foot inward.
- The anterior tibialis pulls the ankle upward.
Nerves
The nerve supply of the ankle is from nerves that pass by the ankle on their way into the foot. The tibial nerve runs behind the medial malleolus. Another nerve crosses in front of the ankle on its way to top of the foot. There is also a nerve that passes along the outer edge of the ankle. The nerves on the front and outer edge of the ankle control the muscles in this area, and they give sensation to the top and outside edge of the foot.
Blood Vessels
The ankle gets blood from nearby arteries that pass by the ankle on their way to the foot. The dorsalis pedis runs in front of the ankle to the top of the foot. (You can feel your pulse where this artery runs in the middle of the top of the foot.) Another large artery, called the posterior tibial artery, runs behind the medial malleolus. It sends smaller blood vessels to the inside edge of the ankle joint. Other less important arteries entering the foot from other directions also supply blood to the ankle.
A bunionette is similar to a bunion, but it develops on the outside of the foot. It is sometimes referred to as a tailor’s bunion because tailors once sat cross-legged all day with the outside edge of their feet rubbing on the ground. This produced a pressure area and callus at the bottom of the fifth toe.
Anatomy
Where does a bunionette develop?
A bunionette occurs over the area of the foot where the small toe connects to the foot. This area is called themetatarsophalangeal joint, or MTP joint. The metatarsals are the long bones of the foot. The phalanges are the small bones in each toe. The big toe has two phalanges, and the other toes have three phalanges each.
Causes
How does a bunionette develop?
Today a bunionette is most likely caused by an abnormal bump over the end of the fifth metatarsal (the metatarsal head) rubbing on shoes that are too narrow. Some people’s feet widen as they grow older, until the foot splays. This can cause a bunion on one side of the foot and a bunionette on the other if they continue to wear shoes that are too narrow. The constant pressure produces a callus and a thickening of the tissues over the bump, leading to a painful knob on the outside of the foot.
Many problems that occur in the feet are the result of abnormal pressure or rubbing. One way of understanding what happens in the foot as a result of abnormal pressure is to view the foot simply. Essentially a foot is made up of hard bone covered by soft tissue that we then put a shoe on top of. Most of the symptoms that develop over time are because the skin and soft tissue are caught between the hard bone on the inside and the hard shoe on the outside.
Any prominence, or bump, in the bone will make the situation even worse over the bump. Skin responds to constant rubbing and pressure by forming a callus. The soft tissues underneath the skin respond to the constant pressure and rubbing by growing thicker. Both the thick callus and the thick soft tissues under it are irritated and painful. The answer to decreasing the pain is to remove the pressure. The pressure can be reduced from the outside by changing the pressure from the shoes. The pressure can be reduced from the inside by surgically removing any bony prominence.
Symptoms
What do bunionettes feel like?
The symptoms of a bunionette include pain and difficulty buying shoes that will not cause pain around the deformity. The swelling in the area causes a visible bump that some people find unsightly.
Diagnosis
How do doctors identify a bunionette?
The diagnosis of a bunionette is usually obvious on physical examination. X-rays may help to see if the foot has splayed and will help decide what needs to be done if surgery is necessary later.
Osteochondritis dissecans (OCD) is a problem that causes pain and stiffness of the ankle joint. It can occur in all age groups. Most cases of OCD usually follow a twisting injury to the ankle and are actually fractures of the joint surface.
Anatomy
Where does OCD develop?
The talus is one of the large bones in the back part of the foot that helps form the ankle joint. The area where OCD occurs is located at the top of the talus. Depending on how the ankle is injured, the problem can occur on the side of the talus closest to the other foot or on the outside part.
The top of the talus is part of the joint and is covered with articular cartilage, the white, slippery material that covers all joint surfaces. On the talus, this covering is about one-eighth of an inch thick. This material allows the bones of the joint to slide against each other without much friction. Right below the articular cartilage is the bone of the talus.
Causes
How does OCD develop?
The cause of most cases of OCD are thought to be actual chip-type fractures. These fractures occur with severe ankle sprains. Which side of the talus the chip is on depends on how the ankle was twisted during the initial injury.
The chip fracture can vary in size and severity. If the bone underneath the cartilage is crushed or cracked and the articular cartilage is intact, the fragment is less likely to move. If the articular cartilage is broken as well, the bone fragment may move out of position, or displace, making healing less likely and later problems more likely.
Because the bone chip is separated from the rest of the talus, the blood vessels traveling to the fragment through the bone of the talus are torn, and the blood supply of the bone fragment is lost. If the fragment displaces, these blood vessels cannot grow back. The fragment loses its blood supply and actually dies. This makes healing less likely. There is some evidence that the twisting injury may not cause a chip fracture initially. However, it may injure the bone’s blood supply, leading to an area of the bone actually dying. This may explain some cases of OCD that appear without a well-defined history of a recent serious twisting injury.
Symptoms
What does OCD feel like?
Initially, OCD behaves like any other ankle sprain injury. You will feel swelling and pain and have difficulty placing weight on the ankle. No special symptoms suggest a chip fracture has occurred inside the joint. X-rays are the best way to determine whether a chip fracture has occurred.
Later, continued problems with the fragment may cause swelling and a generalized ache in the ankle. You may also feel a catching sensation with the ankle in certain positions. This is because the chip can get caught in the ankle joint as it moves, causing pain and the sensation of catching.
Diagnosis
How will the doctor know it’s OCD?
The diagnosis of OCD may be suggested by the history and physical examination. X-rays of the ankle will usually show a problem on the top of the talus (sometimes called the talar dome). Special tests such as a computerized tomography (CT) or a magnetic resonance imaging (MRI) scan may be necessary to determine the full extent of the area involved.
Hallux rigidus is a degenerative type of arthritis that affects the large joint at the base of the big toe. Degenerative arthritis results from wear and tear on the joint surface over time. The condition may follow an injury to the joint or, in some cases, may arise without a well-defined injury.
Anatomy
Where does hallux rigidus occur?
The joint at the base of the big toe is called the metatarsophalangeal, or MTP, joint. Like any other joint in the body, the joint is covered with articular cartilage, a slick, shiny covering on the end of the bone. If this material is injured, it begins a slow process of wearing out, or degeneration. The articular surface can wear away until raw bone rubs against raw bone.
Bone spurs form around the joint as part of the degenerative process. The spurs, or bony outgrowths, may restrict the motion in the joint, especially the ability of the toe to bend upward when the foot moves forward.
Causes
Why do I have this problem?
Doctors remain uncertain about the true cause of hallux rigidus. Many surgeons feel that, in many cases, the condition begins with an injury to the articular cartilage lining the joint, such as from stubbing the big toe. The injury sets in motion a degenerative process that may last for years before symptoms occur that need treatment.
The condition can occur in younger adults but most often affects those who are 50 years old or older. Women seem to develop this problem more often than men. There may be a hereditary factor since two-thirds of patients have a positive family history. Patients who have other family members with hallux rigidus tend to have the problem in both feet (bilateral).
Other cases of hallux rigidus seem to arise without any type of serious injury. This suggests that there may be other reasons for the development of the condition. Minor differences in the anatomy of the foot may make it more likely that certain individuals develop hallux rigidus. This could be a slight change in the shape of the end of the bone (e.g., flatter than normal or oddly-shaped). The fascia (connective tissue) under the foot may be contracted (tight) increasing pressure on the MTP joint. These minor abnormalities may increase the stress that is placed on the joint while walking. Over many years, this may add up to degenerative arthritis of the joint.
Symptoms
What does hallux rigidus feel like?
The degeneration causes two problems–pain and loss of motion in the MTP joint. Without the ability of the MTP to move enough to allow the foot to roll through a full step, walking can become painful and difficult. Pain is most noticeable just before toe-off. Pain is increased when wearing shoes that have elevated heels. Bone spurs that develop with this condition can also put pressure on nearby nerves, causing numbness along the inside edge of the big toe.
Diagnosis
How do doctors identify the problem?
Diagnosis is usually apparent on physical examination, but X-rays are usually required to appreciate the extent of the degeneration and bone spur formation. X-rays also show the shape of the metatarsal head, amount of joint space, and presence of cartilage loss. This information can help direct treatment. MRIs or CT scans are only needed when the X-rays come back normal but some type of lesion is suspected.
Cuboid syndrome is a condition characterized by subluxation (partial dislocation) of the cuboid bone in the foot (figure 1).
The foot comprises of many small bones, one of which is the cuboid (figure 1). The cuboid bone is situated at the outer aspect of the mid-foot and is connected to adjacent bones via strong connective tissue forming joints. These joints provide outer foot stability and allow movement to take place.
During weight bearing activity, certain movements of the foot and ankle and contraction of certain muscles of the lower leg and foot (e.g. peroneus longus), stress is placed on the cuboid bone and surrounding soft tissue. If these forces are excessive and beyond what the bone and surrounding soft tissue can withstand, tearing of the supportive connective tissue may occur. This may allow the cuboid bone to sublux or partially move out of its normal alignment relative to the adjacent foot bones. When this occurs, the condition is known as cuboid syndrome.
Causes of cuboid syndrome
Cuboid syndrome may develop due to excessive traction on the cuboid due to repetitive contraction of the peroneus longus muscle (figure 2). This may occur in association with Peroneus Longus Tendinopathy. Cuboid syndrome may also develop following a Sprained Ankle whereby the foot and ankle are turned inward excessively (inversion), therefore causing damage to the connective tissue holding the cuboid bone in position. Most patients who develop this condition have excessively pronated feet (flat feet) although the condition may also be seen in those with lateral ankle instability. Cuboid syndrome is particularly common in ballet dancers and runners.
Signs and symptoms of cuboid syndrome
Patients with cuboid syndrome usually experience outer (lateral) foot pain that increases with weight bearing forces through the outer foot and may cause weakness during the push off phase of walking. Pain will often increase with twisting or unguarded movements or with running (particularly on hard surfaces and in unsupportive shoes). Pain may radiate into the sole of the foot, the front of the ankle or into the toes. In more severe cases, the patient may limp or walk with an abnormal gait (e.g. walk on their toes) in attempt to reduce stress on the cuboid bone. Pain may also increase on firm palpation of the cuboid bone. Rest from weight-bearing activity usually eases symptoms, unless significant inflammation is involved. Pain upon initial weight-bearing in the morning is also common.
Diagnosis of cuboid syndrome
A thorough subjective and objective examination from a physiotherapist or doctor is important to assist with diagnosis of cuboid syndrome. Investigations such as an X-ray, MRI, CT scan, bone scan or ultrasound may be required in some cases to confirm diagnosis and rule out other injuries.
A Patient’s Guide to Ankle Syndesmosis Injuries
Introduction
An ankle injury common to athletes is the ankle syndesmosis injury. This type of injury is sometimes called a high ankle sprain because it involves the ligaments above the ankle joint. In an ankle syndesmosis injury, at least one of the ligaments connecting the bottom ends of the tibia and fibula bones (the lower leg bones) is sprained. Recovering from even mild injuries of this type takes at least twice as long as from a typical ankle sprain.
Anatomy
What part of the ankle is involved?
A syndesmosis is a joint where the rough edges of two bones are held together by thick connective ligaments. The connection of the lower leg bones, the tibia and fibula, is a syndesmosis. The tibia is the main bone of the lower leg. The fibula is the small, thin bone that runs down the outer edge of the tibia.
Only a few joints in the body are syndesmosis joints. In addition to the ankle syndesmosis (the connection of the tibia and fibula), syndesmosis joints are also located in the lower spine, where the top of the triangular-shaped sacrum bone fits between the pelvis bones. Most joints in the body are synovial joints. Synovial joints are enclosed by a ligament capsule and contain a fluid, called synovium, that lubricates the joint. The ankle syndesmosis sits next to the ankle synovial joint, where the tibia meets the talus bone.
The ankle syndesmosis is supported and held together by three main ligaments. The ligament crossing just above the front of the ankle and connecting the tibia to the fibula is called the anterior inferior tibiofibular ligament (AITFL). The posterior fibular ligaments attach across the back of the tibia and fibula. These ligaments include the posterior inferior tibiofibular ligament (PITFL) and the transverse ligament. The interosseous ligament lies between the tibia and fibula. (Interosseous means between bones.) The interosseus ligament is a long sheet of connective tissue that connects the entire length of the tibia and fibula, from the knee to the ankle.
The syndesmosis ligaments hold the bottom ends of the tibia and fibula in place. This arrangement forms the upper surface of the ankle joint. The ankle joint is a hinge joint. The hinge is formed where the tibia and fibula sit above the talus bone. This connection is called a mortise and tenon, a stable connection that woodworkers and craftsmen routinely use to create strong and stable constructions.
Causes
Why do I have this problem?
Doctors do not completely understand how syndesmosis injuries occur, though they appear to happen most often when the foot is forced upward and outward. Such injuries frequently happen in high-level football players, although snow skiers also account for a high percentage of syndesmosis injuries.
Many times, a patient describes having sprained an ankle. It isn’t until later, when standard treatments for the ankle sprain aren’t helping, that further testing shows a syndesmosis injury.
An ankle syndesmosis injury involves a sprain of one or more of the ligaments that support the ankle syndesmosis. A ligament is made up of multiple strands of connective tissue, similar to a nylon rope. A sprain stretches or tears the ligaments. Minor sprains only stretch the ligament. A tear may be either a complete tear of all the strands of the ligament or a partial tear of only some of the strands. The ligament is weakened by the injury. How much it is weakened depends on the degree of the sprain.
Mild syndesmosis sprains usually involve a stretch or slight tear in only one of the ligaments making up the syndesmosis. Moderate tears of the ankle syndesmosis may lead to ankle joint instability, which make the ankle mortise loose. In severe tears of the ligaments, the ends of the tibia and fibula actually spread apart. This condition is called diastasis.
Symptoms
What does an ankle syndesmosis injury feel like?
Syndesmosis injuries are the most severe sprains of the foot and ankle. They also cause the most problems for people trying to get back to normal activity, especially athletes hoping to resume intense running, cutting, and jumping.
Mild to moderate syndesmosis sprains may at first feel like a routine sprained ankle. Symptoms include pain and swelling on the outside of the ankle.
If the problem has been ongoing, patients may have pain due to an unstable ankle joint. They may feel vague pain around the ankle. Attempts to turn or twist the injured foot may cause sharp pain in the ankle joint. Pain may radiate upward along the side of the lower leg. And the ankle may feel weak, like it can’t be trusted to hold steady, even during routine activities.
Diagnosis
How do doctors diagnose the condition?
The diagnosis of syndesmosis injuries is usually made by examining the ankle. The doctor moves your ankle in different positions in order to check the ligaments and tendons around the ankle. The syndesmosis is stressed by turning the ankle outward while holding the lower leg still. Another test, called thesqueeze test, is done by grabbing the calf just above the ankle joint and squeezing it. Pain with this test is a hallmark of a syndesmosis injury.
Tenderness can usually be pinpointed over the front ankle ligaments (the AITFL) and possibly over the posterior fibular ligaments (the PITFL and transverse ligaments).
X-rays are used to determine the severity of the syndesmosis injury. Stress X-rays are done to see if the tibia and fibula splay apart. The stress X-ray is done with the foot angled outward. An enlarged gap between the tibia and fibula indicates a diastasis (mentioned earlier). X-rays are also used to check for other problems, such as a fracture in the leg or ankle.
Doctors usually suspect a syndesmosis injury when patients have severe pain that lingers after what was thought to be a routine ankle sprain.

I
Ingrown toenail is a condition that most commonly affects the hallux, or big toe. This condition usually results when pressure from improper shoe wear and improper care of the toenails leads to pain and overgrowth of the tissue at the side of the nail.
Anatomy
How does a toenail normally grow?
The toenail (and any other nail) is produced by the nail’s germinal matrix (special nail-generating tissue) and grows forward to the end of the toe. Most of us have lost either a fingernail or toenail and watched as the nail regrew slowly over several months. The area under the nail that attaches the nail to the toe is called the sterile matrix. The sterile matrix doesn’t produce the nail. The sterile matrix just attaches the nail to the toe. On either side of the nail is an area called the nail groove, where the skin of the toe meets the nail matrix and the edge of the toenail.
Causes
How does the problem develop?
In the case of the ingrown toenail, the nail groove begins to disappear, probably due to pressure from ill fitting shoes. The chronic pressure of the nail edge rubbing against the nail groove causes irritation and swelling of the surrounding skin. If the condition continues, hypertrophy, or overgrowth, of the tissue, leads to permanent changes in the tissue. These changes only make the situation worse. Eventually, an infection can occur in the area, leading to even more pain and swelling. Improper trimming of the toenail can also cause problems. If the corner of the toenail is not allowed to grow out past the skin at the end of the nail groove, it may dig into the skin. This makes the pressure from the shoe even more painful.
Symptoms
What does an ingrown toenail feel like?
The primary symptom of an ingrown toenail is pain. The toe is red and painful to the touch, and it can be difficult to wear shoes. If infection is present, pus may drain from the area as well.
Diagnosis
How will my doctor confirm it’s an ingrown toenail?
Diagnosis is generally easily made on examination. No X-rays or tests are usually required, unless your doctor suspects that the infection may have spread to the bone.